
What are fibroids?

Fibroid being removed at surgery
Fibroids are benign tumours of the uterus (womb). They are not cancerous and so are very unlikely to be a threat to life. Fibroids are however very common affecting about half of all women at some stage in their lives. Though most women with fibroids have no symptoms and may not even know they have them, a minority suffer very distressing symptoms.
Fibroids are made up of muscle and are very vascular i.e. have a large supply of blood to them. No-one knows for sure what causes fibroids but they are certainly influenced by hormones and most likely to grow faster when oestrogen is highest in a woman’s middle life.They are rare in teenagers, most common in 30-50 year olds and shrink naturally after the menopause.
Fibroids are much more common in black women than white women. Your chance of developing them is also increased if you are heavy, if other members of your family have been diagnosed with them, or if you have no children. Fibroids vary considerably in size and number; some may be the size of a marble others are like a large pumpkin.
Fibroids can affect a woman’s life very profoundly. Their affect and the effect of their treatment vary considerably from one patient to another. Although fibroids are a common problem, however many women have been affected by fibroids before you, your reaction physically and emotionally to the disease and its treatment is unique to you. Take time to assess all the options, talk to your doctors and make sure that you get the treatment that is right for you.
Types of Fibroid
All fibroids are not the same. They occur in different parts of the uterus and their site influences the symptoms they cause. The uterus is basically a bag of muscle, designed with one purpose in mind, to look after and deliver an unborn baby. The muscle in the wall of the uterus is there to help push the baby out of the body when the time is right. The uterus naturally has a tremendous potential to rapidly grow during pregnancy, and equally as rapidly shrink after delivery.


Other important aspects of the uterus are a blood supply (the uterine arteries) which provides nutrition to the uterus itself, but has tremendous potential to increase to support the life and growth of a baby. The interior of the vascular bag of the uterus is lined by a skin called the mucosa, on which the placenta grows, which allows nutrients to pass from the mother’s blood to the baby blood.
Normally the interior of the uterus is collapsed down like the inside of a deflated toy balloon but it can be inflated easily by the presence of a growing baby or by a tumour.
The uterus lies deep down inside the belly, and opens onto the outside world through the cervix or neck of the womb, and then the vagina and vulva. In front of the uterus lies the bladder, and behind the uterus lies bowel (in particular, the rectum) and many nerves. This position in relation to the structures is important to patients with large fibroids as pressure on the structures causes many of the common symptoms of fibroids. The outside of the muscular bag is covered by another layer of skin called serosa.
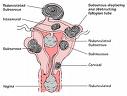
Fibroids can be
- sub-serosal (under the mucosa on the outside of the womb)
- intra-mural (within the wall of the uterus)
- sub-mucosal (under the mucosa on the inside of the uterus)
- cervical (arising from the cervix itself, the neck of the womb)
Fibroids may also be pedunculated – i.e. on a think stalk (hanging like a fruit on a tree. Pedunculated fibroids can be hanging off the outside of the uterus or hanging within the cavity of the uterus.
Many patients have a mixture of these different types of fibroid at the same time.
Can Fibroids be prevented?
There is little that can be done to prevent fibroids occurring, but the risk can be reduced by:-
- Keeping your weight within healthy limits
- Eating a sensible diet with plenty of fresh fruit and vegetables
- Taking the combined oral contraceptive pill (not recommended just to prevent fibroids however).
Infertility and Problems with Pregnancy
Most fibroids do not affect your ability to become pregnant or the pregnancy itself. Some may cause pregnancy to be more uncomfortable than normal. In a minority of women, the fibroids can make conception difficult and can cause miscarriage. This is logical as an abnormal lump in the uterus can easily be imagined to block the fallopian tube preventing the egg travelling from the ovary to the uterus. A fibroid within the lining of the womb is also likely to interfere with the growing embryo and increase the chance that the pregnancy will be lost. Occasionally, a fibroid may lost its blood supply during pregnancy and die. If this happens, it can cause severe pain and can induce a miscarriage or bring on a premature delivery.
At the time of birth, large fibroids can give difficulty by obstructing the passage of the baby. If this occurs, a caesarean section may be necessary. After birth, the fibroids increase the risk of bleeding which can be heavy and may require some form of medical intervention to stop it.
How are Fibroids diagnosed?
Your GP or gynaecologist may have a good idea that you have fibroids from the symptoms that you report and the internal examination he performs. However, to confidently make the diagnosis requires some form of scan. The commonest is an ultrasound scan often undertaken internally (a transvaginal scan).
Ultrasound
An ultrasound scan will be able to give a very accurate idea of whether or not you have fibroids. It cannot indicate for certain if the fibroids are responsible for the symptoms you are experiencing.
Magnetic resonance
 Once fibroids are diagnosed and before deciding on which treatment is appropriate, a magnetic resonance scan may be arranged. This is a special form of scan which is not dangerous, as it involves no x-rays, but it is expensive, takes some time, and you may find it claustrophobic. Magnetic resonance scans give exquisite detail of the anatomy of your lower belly. They can show exactly how many fibroids you have, how big they are, how vascular they are (how much blood supply they have), whether they are dead or alive (some fibroids die off naturally), where they are (sub-mucous, sub-serosal, intra-mural), whether they are pedunculated and very importantly, if there is any indication of other pathology which may be relevant to the management of your problems. Magnetic Resonance is much more accurate than ultrasound and can often correct a misdiagnosis of fibroids given by an ultrasound scan, and change the appropriate treatment. You will be able to look at the magnetic resonance image and see for yourself what the fibroids look like, and understand why they may be causing you problems.
Once fibroids are diagnosed and before deciding on which treatment is appropriate, a magnetic resonance scan may be arranged. This is a special form of scan which is not dangerous, as it involves no x-rays, but it is expensive, takes some time, and you may find it claustrophobic. Magnetic resonance scans give exquisite detail of the anatomy of your lower belly. They can show exactly how many fibroids you have, how big they are, how vascular they are (how much blood supply they have), whether they are dead or alive (some fibroids die off naturally), where they are (sub-mucous, sub-serosal, intra-mural), whether they are pedunculated and very importantly, if there is any indication of other pathology which may be relevant to the management of your problems. Magnetic Resonance is much more accurate than ultrasound and can often correct a misdiagnosis of fibroids given by an ultrasound scan, and change the appropriate treatment. You will be able to look at the magnetic resonance image and see for yourself what the fibroids look like, and understand why they may be causing you problems.
Hysteroscopy
Particularly if your problem is menorrhagia (excessive bleeding), your gynaecologist may recommend looking directly into the inside of your womb with a hysteroscope. This is a small camera which can be inserted into the womb through the cervix. This can usually be done without need for general anaesthesia. It gives a direct view of the lining of the womb and can be useful for diagnosing sub-mucosal fibroids. It cannot see fibroids within the body of the womb (intra-mural) or sub-serous fibroids, though the gynaecologist may get an idea of the presence of other fibroids if the cavity is distorted. A biopsy of the lining of the womb can be taken at the time of the hysteroscopy.
Laparoscopy
 Hysteroscopy looks into the inside of the womb. Laparoscopy uses a similar camera, but inserted through a small cut in the abdominal wall and looks at the uterus and other pelvic organs from the outside. It is undertaken under a general anaesthetic. It is good at detecting other problems, but is rarely indicated to diagnose fibroids.
Hysteroscopy looks into the inside of the womb. Laparoscopy uses a similar camera, but inserted through a small cut in the abdominal wall and looks at the uterus and other pelvic organs from the outside. It is undertaken under a general anaesthetic. It is good at detecting other problems, but is rarely indicated to diagnose fibroids.
Treatment options for Fibroids
Once the diagnosis is accurately established with the magnetic resonance scan, a range of different treatment options is available for patients whose fibroids are causing problems. Remember before considering treatment to always weigh up the risks of treatment against the potential benefits. No medical treatment is totally risk free, and if your fibroids are causing no problems, it would be silly to take any risk however small. Also consider what the likely progression of your problem is. If for example you are nearing the menopause then it is likely that the fibroids will naturally get smaller and your symptoms naturally improve. The options for active treatment nowadays are many and varied including drugs, surgery, UAE, magnetic resonance and HIFU (high intensity focused ultrasound).
Drugs
Drugs are available which reduce oestrogen levels and cause fibroids to shrink. A six month course can reduce the fibroid by up to 50% and reduce many of the symptoms. The drugs stop your normal periods. They can, however, only be taken for about six months. After this time, the fibroids often start growing again and causing more symptoms. The drugs themselves can cause side effect including hot flushes and vaginal dryness. Drugs may be very helpful in patients nearing the menopause, but are unlikely to be a good solution for younger women with large symptomatic fibroids. They may be helpful in making surgery easier and safer.
 Surgery
Surgery
This has traditionally been the most common form of treatment for fibroids, and huge numbers of women used to undergo hysterectomy (removal of the womb) for this reason. Hysterectomy is not however the only surgical option. The fibroids themselves can be removed leaving the uterus intact (myomectomy). This can be performed through normal surgery or with keyhole techniques.
Hysterectomy
Hysterectomy is the surgical removal of the womb. It used to be one of the commonest operations performed in the United Kingdom and many of these were for fibroids. The obvious advantage of a hysterectomy is that once the uterus is removed, there is no chance of fibroids returning. They are gone forever. However, it is major surgery involving several days in hospital for most patients and several weeks of recuperation. It is not without risk, and hysterectomy for fibroids is more risky than hysterectomy for most other conditions. There are several different ways to perform a hysterectomy which can be confusing. Traditionally, it is performed through an incision in the lower belly (abdominal hysterectomy), but in some cases it can be performed through the vagina (vaginal hysterectomy) without involving any cuts or scars on the belly. In general, vaginal hysterectomy can only be performed if the fibroids are small. Newer, less invasive methods of performing a hysterectomy have been developed with a view to reducing post operative recovery time, complications and side effects. These include: – laparoscopic assisted vaginal hysterectomy, laparoscopic supra-cervical hysterectomy and total laparoscopic hysterectomy. Despite the intention of these minimally invasive alternatives to traditional surgery, there is evidence that they are in fact riskier than traditional methods. This may, however, be due to lack of surgeon’s experience with laparoscopic methods compared to traditional methods and this may change with increased experience.
Hysterectomy usually requires at least eight weeks off work and one third of patients will suffer a complication. Well known major complications include haemorrhage and injury to bowel, ureter, bladder, pulmonary embolus, unintended conversion of laparoscopy to laparotomy, wound breakdown. The obvious advantage of hysterectomy over other treatments is that the fibroids will never come back. The obvious disadvantage is that future pregnancies are impossible. This of course for some patients may be seen as a distinct advantage.
Myomectomy
Myomectomy is the surgical removal of the fibroids themselves, leaving the uterus intact. They can be performed through an incision in the body or laparoscopically through instruments inserted through small incisions. Both require general anaesthesia. Recovery time is less than for a hysterectomy with about four weeks of normal activity. There is a chance that fibroids can grow back after myomectomy (estimated 10-15%). This figure is probably much higher in black women. Pregnancy is possible after myomectomy but there is a concern that the scars on the uterus could pose problems with future pregnancies and ability to conceive. About 20% of patients having a myomectomy later need to have a hysterectomy either as a result of complications or lack of sufficient symptom relief. Myomectomy performed using a laparoscope is available in some hospitals. Although this surgery is more time consuming than traditional myomectomy, the recovery time is reduced with most returning to near normal activities after fourteen days. With any myomectomy technique it is rare to be available to remove all the fibroids and those left behind are likely to grow. New fibroids may also develop in the normal uterus left behind. It should be possible to become pregnant after a myomectomy. Small sub-mucous fibroids may be removed using a hysteroscope inserted through the vagina and cervix. This can be performed under a local anaesthetic or more usually a general anaesthetic. It is usually performed as a day case procedure and you need to rest for at least a week. As with other forms of myomectomy, there is a chance (20%) of the fibroids coming back but you should be able to retain your fertility.
UAE (uterine artery embolisation)
UAE is an established minimally invasive treatment which avoids the need for surgery and anaesthesia and which is very popular with many patients.
Uterine Artery Embolisation (UAE)
 UAE or uterine artery embolisation is a relatively new procedure in which the blood supply to the fibroids is blocked off causing the fibroids to shrink.
UAE or uterine artery embolisation is a relatively new procedure in which the blood supply to the fibroids is blocked off causing the fibroids to shrink.
This treatment is carried out by an interventional radiologist rather than a gynaecologist.
A typical interventional radiology operating theatre
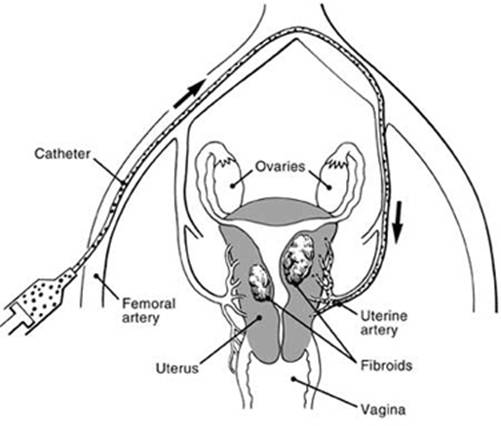
UAE involves the deliberate blockage of the blood supply to the fibroids by injecting particles of glue into the arteries via a small plastic tube (catheter) inserted through a pinhole incision into the main artery in the groin.
UAE has been used for many years to stop bleeding from the uterus in the mothers who have just given birth. In the early 1990’s, it was first used in France as a treatment for Fibroids and very quickly it was taken up by radiologists especially in the USA. It has had a slower uptake in the UK, but now is available in most large hospitals. Using local rather than general anaesthesia, a catheter about 1.5mms wide is threaded into the main artery in the groin through a pinhole incision. This catheter is then guided into position within each uterine artery in turn left and right. Once in position, particles of PVA glue are injected to block off the blood supply.
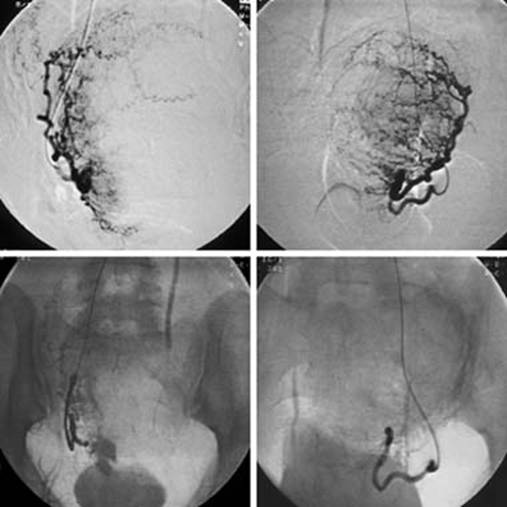
Xrays taken during an embolisation treatment showing the blood supply
before the embolisation (above) and after (below)
The fibroid, thus deprived of its blood supply usually shrivels up and dies.
PVA glue is used in many different treatments and has been proven to be an entirely safe substance for use in the human body.
The procedure takes about thirty minutes to perform. The catheter is then removed from the groin artery and pressure applied for ten minutes to close the wound. No stitches are needed. The patient then goes back to the ward to recover. The procedure is usually painless, but soon after the procedure, pains start which normally last for about 24 hours. During this time, the patient is given control of a morphine pump to take on demand powerful painkillers to numb any pain. An anti-inflammatory suppository is also given just prior to the procedure which is also very effective in reducing pain. Patients are usually able to go home the day following the procedure and can get back to work after a week or two. They normally feel totally normal after two weeks, but in the meantime may experience cramping pains and suffer from irregular bleeding. A raised temperature is also common and is a natural reaction to the killing of tissue in the body. The fibroids shrink gradually over six months and symptoms may continue to improve over this time.
Results of UAE
Success rate of UAE is over 85%. UAE kills all fibroids in one go with a very low recurrence rate long term. There is a risk of complication as with any medical treatment but the risk is low. There is a 1 in 200 chance of needing a hysterectomy as a result of complication (usually infection). Ovarian failure is another important complication occurring in 1% of patients under 45 years of age. There is a very low risk of death. Five patients worldwide have been reported to have died and over 100,000 procedures have been performed. Two of the deaths were from pulmonary embolus and three from infection. The complication rate of UAE is much lower than hysterectomy for fibroids which has a serious complication rate of 5% and a death rate of 1 in 1,500. Satisfaction rates for the procedure are over 90%.
Pregnancy after UAE
There is limited information about pregnancy after UAE, but a recent study of 56 completed pregnancies showed that:-
- 30% of patients wishing to become pregnant achieved pregnancy
- 60% of these resulted in a live birth
- 18% of these were premature
- 30% had miscarriages
- 2% had stillbirths
- 18% had post partum haemorrhage
- 72% had caesarean section
All these figures are poorer than the general population. Very careful consideration needs to be made of the potential problems with future pregnancies before deciding to undergo UFE. If you hope to become pregnant you should talk to both your gynaecologist and interventional radiologist about the implications to you and your baby
NICE guidance on heavy menstrual bleeding and Fibroids
This recommends referral for consideration for surgery (myomectomy or hysterectomy) or UAE. All these techniques should be discussed with the patient. Women should be informed that UAE or myomectomy may potentially allow them to retain their fertility. Myomectomy is recommended for women with heavy menstrual bleeding associated with fibroids who want to retain their uterus. UAE is recommended for women with heavy menstrual bleeding associated with fibroids and who want to retain their uterus and/or avoid uterus. Hysterectomy should be considered only when:-
- Other treatment options have failed, are contra-indicated or declined
- There is a wish for amenorrhoea
- The woman requests it
- The woman no longer wishes to retain her uterus and fertility.
Women offered hysterectomy should have a full discussion of the implications of surgery before a decision is made. This discussion should include sexual feelings, fertility impact, bladder function, need for further treatment, treatment complications, a woman’s expectations, alternative surgery and psychological impact.
Women offered hysterectomy should be informed about the increased risk of serious complications (such as intra-operative haemorrhage, or damage to other organs) associated with hysterectomy when uterine fibroids are present. Women should be informed about the risk of possible loss of ovarian functions and its consequences if their ovaries are retained during hysterectomy. The type of hysterectomy that should be considered in the following order:-
- Vaginal
- Abdominal
The laparoscopic approach should be considered in certain circumstances e.g. morbid obesity. If abdominal hysterectomy is decided upon, then both the total method (removal of uterus and cervix) and sub-total method (preservation of the cervix) should be discussed.
NICE guidance on UAE
It has been decided that the procedure is safe enough and that most patients have improved symptoms. All patients should be given full information about the treatment and any uncertainties e.g. in regard to future pregnancy. The decision on treatment should be made by both a gynaecologist and an interventional radiologist.
Other new techniques for Fibroids which preserve the uterus
There is much research going on with various new techniques including magnetic resonance guided HIFU (high intensity focused ultrasound), MR guided laser treatment and laparoscopic laser myomectomy.
Laparoscopic laser Myomectomy
This involves passing a small endoscope through tiny incisions in the abdominal wall into the lower abdomen. A laser is then directed onto the fibroids to destroy them. It is carried out under general anaethetic. NICE has issued guidance that there are still uncertainties about the safety of the procedure and how well it works. A full discussion of the current evidence for this procedure should take place between the patient and the doctor before consenting to such treatment.
MR Guided HIFU (High Intensity Focused Ultrasound)
This is a new technique in which high intensity ultrasound energy is transmitted without cuts directly through the abdominal wall onto the fibroid with the intention of shrinking them and relieving symptoms. The procedure is undertaken without anaesthetic but some sedation may be given. A limited number of procedures have been carried out to date showing promising results with nearly 90% of patients symptoms significantly improved. Symptoms seem to respond better than reduction in fibroid size. No serious complications have been reported, but less serious complications have included skin burns, ulcerations, sciatica, fatigue, back ache. NICE have issued guidance that it cannot be routinely used in the NHS but can be carried out under special conditions of audit or research. It may have a role in the future but at present is not a routine treatment option.
MR guided Percutaneous Laser Ablation of Fibroids
Needles are inserted through small nicks in the abdomen into the fibroids under local anaesthetic and guided by magnetic resonance scans. A laser fibre is passed through these needles and the fibroid heated to destroy them. Short term reduction in fibroid volume of 30% has been demonstrated at three months. Complications have included skin burns, urinary tract infections and vaginal bleeding.
Although this shows promise for the future NICE has issued guidance stating that there is insufficient evidence to support the use of this procedure unless as part of an audit or research programme.
How much does UAE cost?
UAE is available free on the NHS in most major hospitals in the UK. If you wish to have it performed privately the usual cost is between £3000 and £5000.
References
- Stewart EA, Rabinovici J, Tempany CM, Inbar Y, Regan L, Gostout B, et al. Clinical outcomes of focused ultrasound surgery for the treatment of uterine fibroids. Fertil Steril 2006;85:22-9
- Mara M, Fucikova Z, Maskova J, Kuzel D, Haakova L. Uterine fibroid embolization versus myomectomy in women wishing to preserve fertility: preliminary results of a randomized controlled trial. Eur J Obstet Gynecol Reprod Biol 2006;126:226-33
- National Institute for Health and Clinical Excellence. Heavy menstrual bleeding. NICE guideline CG44. London: NICE, 2007.
- Royal College of Obstetricians and Gynaecologists/Royal College of Radiologists. Clinical recommendations on the use of uterine artery embolisation in the management of fibroids. Report of a joint working party, 2000.
- Ravina JH, Merland JJ, Ciraru-Vigneron N, Bouret JM, Herbreteau D, Houdart E, et al. Arterial embolization: a new treatment of menorrhagia in uterine fibroma. Presse Med 1995;24:1754
- Walker WJ, Pelage JP. Uterine artery embolisation for symptomatic fibroids: clinical results in 400 women with imaging follow up. BJOG 2003;110:1139
- Spies JB, Myers ER, Worthington-Kirsch R, Mulgund J, Goodwin S, Mauro M; Fibroid Registry Investigators. The FIBROID registry: symptom and quality-of-life status 1 year after therapy. Obstet Gynecol 2005;106:1309-18
- Edwards RD, Moss JG, Lumsden MA, Wu O, Murray LS, Twaddle S, et al; Committee of the Randomised Trial of Embolisation versus Surgical Treatment of Fibroids. Uterine artery embolisation versus surgery for symptomatic fibroids. N Engl J Med 2007;356:360-70
- Gupta JK, Sinha AS, Lumsden MA, Hickey M. Uterine artery embolisation for symptomatic fibroids. Cochrane Database Syst Rev 2006;(1):CD005073.
- Hehenkamp WJ, Volkers NA, Donderwinkel PF, de Blok S, Birnie E, Ankum WM, et al. Uterine artery embolisation versus hysterectomy in the treatment of symptomatic fibroids (EMMY trial): peri- and post-procedural results from a randomised controlled trial. Am J Obstet Gynecol 2005;193:1618-29
- Glomset O, Hellesnes J, Heimland N, Hafsahl G, Smith HJ. Assessment of organ radiation dose associated with uterine artery embolisation. Acta Radiol 2006;47:179-85.
